Problems Addressed by BFN
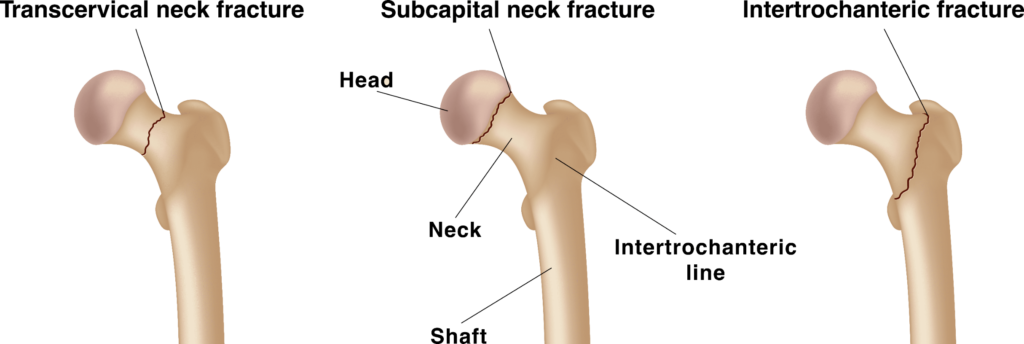
Femoral neck fractures are the most common human bone fractures. In the USA there are estimated to be at least 350,000 femoral neck fractures per year; in Japan there are almost 200,000. The elderly and frail are especially vulnerable to these fractures, which typically result from a fall. As populations age, the number of femoral neck fractures is projected to increase.
Approximately half of femoral neck fractures are treated by intramedullary hip nailing: surgically implanting a short femoral nail (SFN). The SFN, based on Gross’s Gamma Nail, was introduced in 1986 and has not seen major improvement in the intervening 35 years.

short femoral nail (SFN)
Problems with Conventional Short Femoral Nails
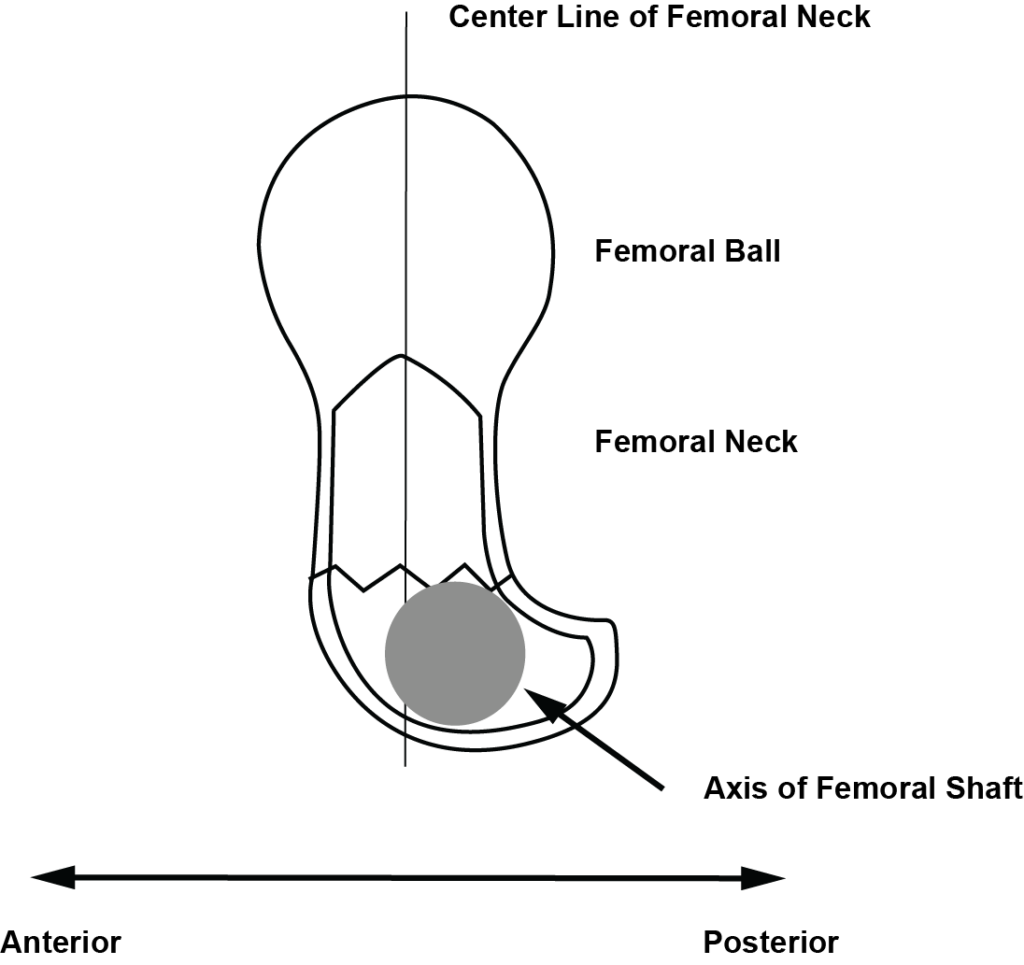
In a conventional SFN, the nail main shaft lies in the same plane as the lag screw. By contrast, in the human femur, the neck and the head of the femur are displaced anterior to the main femoral shaft by approximately 4 mm.
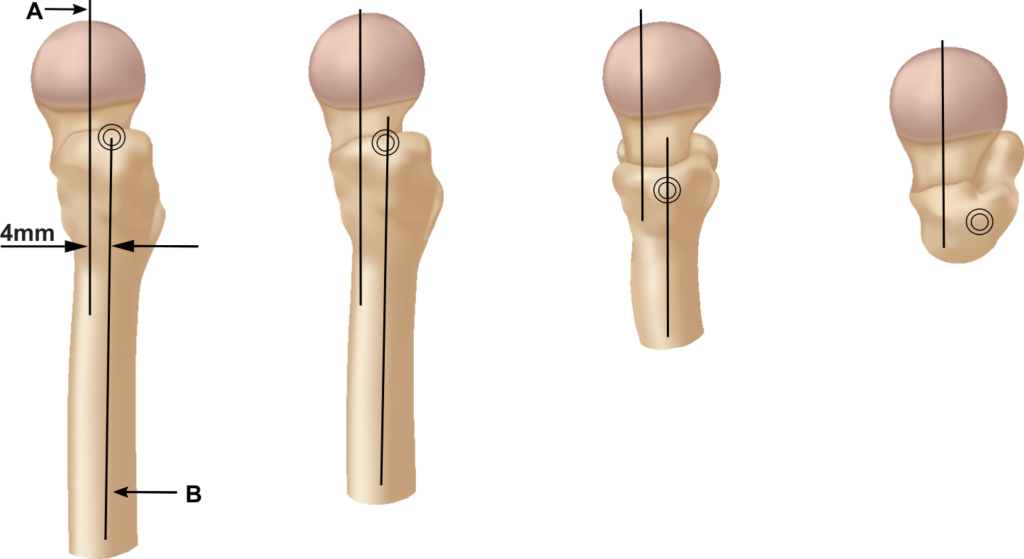
When implanting an SFN, best practice is for the lag screw to pass through center of the femoral neck and for the tip to anchor in the center of the femur ball, in lateral view. However, since the straight SFN does not have the lag screw displace to the anterior of the main nail shaft, in most cases surgery results in either posterior deviation or posterior-anterior (PA) deviation of the lag screw, see figure below.
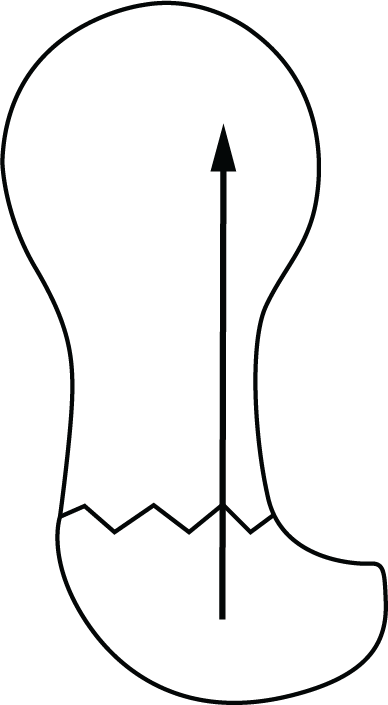
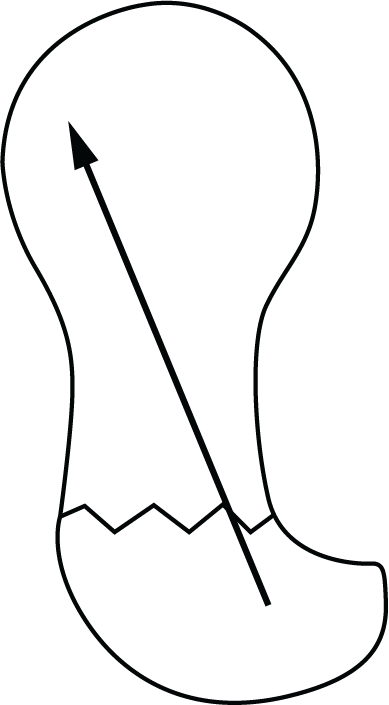
Deviation
Lag Screw Positioning: Central positioning is desired, but surgery often results in posterior or posterior-anterior deviation.
Posterior and posterior-anterior deviations of the lag screw can both cause intramedullary (posterior) displacement of the bones – either intraoperatively, or postoperatively.
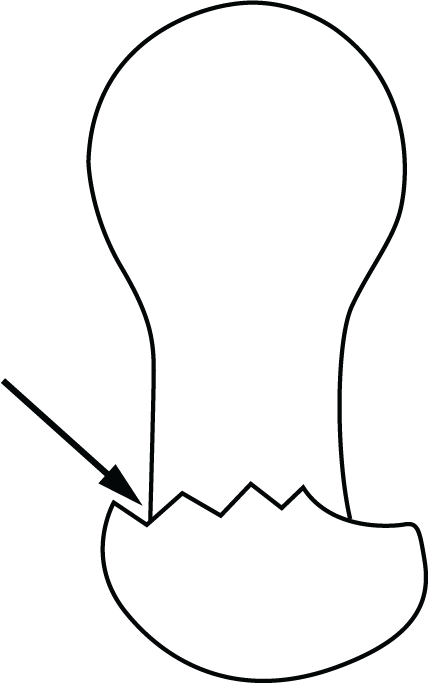
Intramedullary displacement often results in large telescope: the collapse of one bone fragment inside the other. It is estimated that intramedullary displacement occurs in 44% to 82% of cases. Furthermore, intramedullary displacement can cause the lag screw break through the bone surface of the femal ball or femoral neck, a result called “cut-out”.
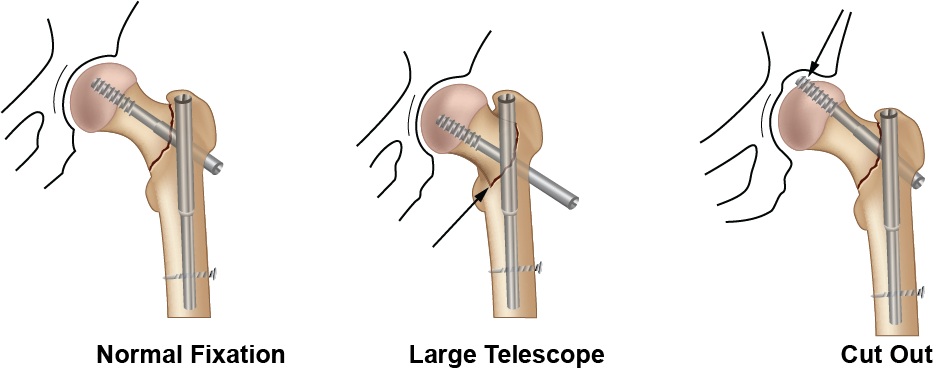
Intramedullary displacement, large telescope, and cut-out lead to poor patient outcomes: longer rehabilitation periods, reduced load bearing capacity, and in some cases need for revision surgery.
BFN Solution
BFN Research developed the Best Fit Nail (BFN) to solve the above problems.
In the BFN, the lag screw is displaced anterior relative to the nail axis. This matches the displacement of the femoral neck and femoral ball relative to the femoral shaft. Therefore, the lag screw is more easily positioned in the center of femoral neck and femoral ball, resulting in anatomical reduction of the fracture.